sciencewithdrdoug.com/2020/08/01/is-a-coronavirus-vaccine-a-ticking-time-bomb/Is a Coronavirus Vaccine a Ticking Time Bomb?Posted byDr. DougAugust 1, 2020Posted inCOVID-19, vaccineTags:ADE, antibody dependent enhancement, coronavirus, coronavirus vaccine, COVID-19, covid19, sars, Sars-cov-2, vaccine
Will a vaccine to SARS-CoV-2 actually make the problem worse? Although not a certainty, all of the current data says that this prospect is a real possibility that needs to be paid careful attention to. If you stay with me, I’ll explain why.
First, let’s set aside the debate surrounding the topic of whether vaccines work and the negative health consequences due to the components of the vaccine. No matter where you stand on the vaccine issue, I’m not asking anyone to capitulate on this point. I’m just asking that this issue be set aside, because in this instance this argument is completely irrelevant. Even without bringing any other issue into the vaccine debate, a coronavirus vaccine is a highly dangerous undertaking due to a peculiar trojan horse mechanism known as Antibody Dependent Enhancement (ADE). Regardless of someone’s conviction about vaccines, this point needs to be acknowledged. In the remaining portion of this article, I’m going to explain how ADE works and the future perils it may bring.
For a vaccine to work, our immune system needs to be stimulated to produce a neutralizing antibody, as opposed to a non-neutralizing antibody. A neutralizing antibody is one that can recognize and bind to some region (‘epitope’) of the virus, and that subsequently results in the virus either not entering or replicating in your cells.
A non-neutralizing antibody is one that can bind to the virus, but for some reason, the antibody fails to neutralize the infectivity of the virus. This can occur, for example, if the antibody doesn’t bind tightly enough to the virus, or the percentage of the surface area of the virus covered by the antibody is too low, or the concentration of the antibody is not high enough. Basically, there is some type of generic binding of the antibody to the virus, but it fails to neutralize the virus.
In some viruses, if a person harbors a non-neutralizing antibody to the virus, a subsequent infection by the virus can cause that person to elicit a more severe reaction to the virus due to the presence of the non-neutralizing antibody. This is not true for all viruses, only particular ones. This is called Antibody Dependent Enhancement (ADE), and is a common problem with Dengue Virus, Ebola Virus, HIV, RSV, and the family of coronaviruses. In fact, this problem of ADE is a major reason why many previous vaccine trials for other coronaviruses failed. Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place.
An antibody can be rendered a non-neutralizing antibody simply because it doesn’t bind to the right portion of the virus to neutralize it, or the antibody binds too weakly to the virus. This can also occur if a neutralizing antibody’s concentration falls over time and is now no longer of sufficient concentration to cause neutralization of the virus. In addition, a neutralizing antibody can subsequently transition to non-neutralizing antibody when encountering a different strain of the virus.
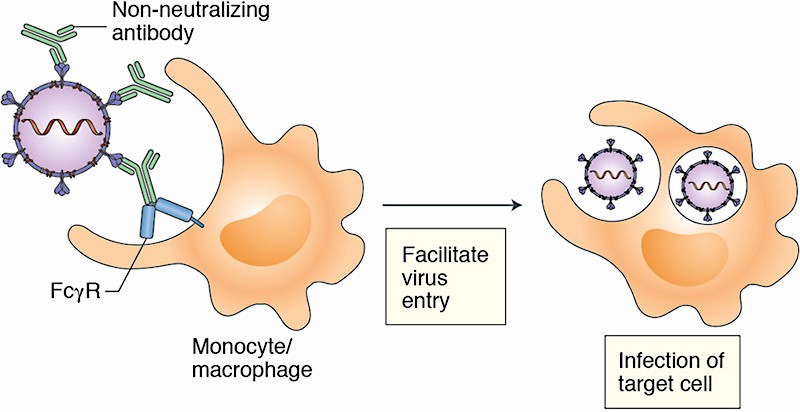
What does ADE entail? The exact mechanism of ADE in SARS is not known, but the leading theory is described as follows: In certain viruses, the binding of a non-neutralizing antibody to the virus can direct the virus to enter and infect your immune cells. This occurs through a receptor called FcγRII. FcγRII is expressed on the outside of many tissues of our body, and in particular, in monocyte derived macrophages, which are a type of white blood cell. In other words, the presence of the non-neutralizing antibody now directs the virus to infect cells of your immune system, and these viruses are then able to replicate in these cells and wreak havoc on your immune response. One end of the antibody grabs onto the virus, and the other end of the antibody grabs onto an immune cell. Essentially, the non-neutralizing antibody enables the virus to hitch a ride to infect immune cells. You can see this in the picture above.
This can cause a hyperinflammatory response, a cytokine storm, and a generally dysregulation of the immune system that allows the virus to cause more damage to our lungs and other organs of our body. In addition, new cell types throughout our body are now susceptible to viral infection due to the additional viral entry pathway facilitated by the FcγRII receptor, which is expressed on many different cell types.
What this means is that you can be given a vaccine, which causes your immune system to produce an antibody to the vaccine, and then when your body is actually challenged with the real pathogen, the infection is much worse than if you had not been vaccinated.
Again, this is not seen in all viruses, or even in all strains of a given virus, and there is a great deal that scientists don’t understand about the complete set of factors that dictate when and if ADE may occur. It’s quite likely that genetic factors as well as the health status of the individual may play a role on modulating this response. That being said, there are many studies (in the reference section below) that demonstrate that ADE is a persistent problem with coronaviruses in general, and in particular, with SARS-related viruses. Less is known, of course, with respect to SARS-CoV-2, but the genetic and structural similarities between the SARS-CoV-2 and the other coronaviruses strongly suggests that this risk is real.
ADE has proven to be a serious challenge with coronavirus vaccines, and this is the primary reason many have failed in early in-vitro or animal trials. For example, rhesus macaques who were vaccinated with the Spike protein of the SARS-CoV virus demonstrated severe acute lung injury when challenged with SARS-CoV, while monkeys who were not vaccinated did not. Similarly, mice who were immunized with one of four different SARS-CoV vaccines showed histopathological changes in the lungs with eosinophil infiltration after being challenged with SARS-CoV virus. This did not occur in the controls that had not been vaccinated. A similar problem occurred in the development of a vaccine for FIPV, which is a feline coronavirus.
For a vaccine to work, vaccine developers will need to find a way to circumvent the ADE problem. This will require a very novel solution, and it may not be achievable, or at the very least, predictable. In addition, the vaccine must not induce ADE in subsequent strains of SARS-CoV-2 that emerge over time, or to other endemic coronaviruses that circulate every year and cause the common cold.
A major trigger for ADE is viral mutation. Changes to the amino acid sequence of the Spike Protein (which is the protein on the virus that facilitates entry into our cells via the ACE2 receptor) can cause antigenic drift. What this means is that an antibody that was once neutralizing can become a non-neutralizing antibody because the antigen has slightly changed. Therefore, mutations in the Spike protein that naturally occur with coronaviruses could presumably result in ADE. Since these future strains are not predictable, it is impossible to predict if ADE will become a problem at a future date.
This inherent unpredictability problem is highlighted in the following scenario: A coronavirus vaccine may not be dangerous initially. If the initial testing looks positive, mass vaccination efforts would presumably be administered to a large portion of the population. In the first year or two, it may appear that there is no real safety issue, and over time, a greater percentage of the world population will be vaccinated due to this perceived “safety”. During this interim period, the virus is busy mutating. Eventually, the antibodies that vaccinated individuals have floating around in their bloodstream are now rendered non-neutralizing because they fail to bind to the virus with the same affinity due to the structural change resulting from the mutation. Declining concentrations of the antibody over time would also contribute to this shift towards non-neutralization. When these previously vaccinate people are infected with this different strain of SARS-CoV-2, they could experience a much more severe reaction to the virus.
Ironically, in this scenario, this vaccine made the virus more pathogenic rather than less pathogenic. This is not something that vaccine producers would be able predict or test for with any level of real confidence at the outset, and it would only become evident at a later time.
If and when this does occur, who will be liable?
Does this vaccine industry know about this problem? The answer is yes, they do.
Quoting a Nature Biotechnology news article published on June 5th, 2020:
““It’s important to talk about it [ADE],” says Gregory Glenn, president of R&D at Novavax, which launched its COVID-19 vaccine trial in May. But “we can’t be overly cautious. People are dying. So we need to be aggressive here.””
And from the same article:
“ADE “is a genuine concern,” says virologist Kevin Gilligan, a senior consultant with Biologics Consulting, who advises thorough safety studies. “Because if the gun is jumped, and a vaccine is widely distributed that is disease enhancing, that would be worse than actually not doing any vaccination at all.””
The vaccine industry is aware of this problem. The degree to which they are taking it seriously, is another question.
While many vaccine developers are aware of the problem, some of them are approaching the problem with more Laissez-faire attitude. They see this problem as “theoretical,” and not guaranteed, with the idea that animal trials should rule out the potential of ADE in humans.
As a side note, it is not ethical to conduct “challenge” studies in humans. However, challenge studies are conducted in animals. In other words, a clinical trial for a vaccine does not include administering the vaccine to a person, and then exposing this person to the virus post-vaccination to monitor their reaction. In clinical trials, humans are only given the vaccine, they are not “challenged” with the virus afterward. In animal studies, they do conduct a challenge test to observe how the animals respond to being infected with the actual virus after being vaccinated.
Will conducting animal studies solve the issue and remove the risk?
Not at all.
Anne De Groot, CEO of EpiVax argues that testing for vaccine safety in primates does not guarantee safety in humans, mainly because primates express different major histocompatibility complex (MHC) molecules, which alters epitope presentation and the immune response. Animals and humans are similar, but they are also very different. In addition, as pointed out above, the development of different viral strains in subsequent years could present a major problem not noticeable during the initial safety trials in either humans or animals.
What about unvaccinated people who are naturally infected with the virus and develop antibodies? Could these people experience ADE to a future strain of SARS-CoV-2?
The ADE response is actually much more complicated than the picture I outlined above. There are other competing and non-competing factors in our immune system that contribute to the ADE response, many of which are not fully understood. Part of that equation is a variety of different types of T-cells that modulate this response, and these T-Cells respond to other portions (epitopes) of the virus. In a vaccine, our body is normally presented with a small part of the virus (like the Spike protein), or a modified (attenuated or dead) virus which is more benign. A vaccine does not expose the entirety of our immune system to the actual virus.
These types of vaccines will only elicit antibodies that recognize the portion of the virus which is present in the vaccine. The other portions of the virus are not represented in the antibody pool. In this scenario, it is much more likely that the vaccine-induced antibodies can be rendered as non-neutralizing antibodies, because the entire virus is not coated in antibodies, only the portion that was used to develop the vaccine.
In a real infection, our immune system is exposed to every nook and cranny of the entire virus, and as such, our immune system develops a panacea of antibodies that recognize different portions of the virus and, therefore, coat more of the virus and neutralize it. In addition, our immune system develops T-Cell responses to hundreds of different peptide epitopes across the virus; whereas in the vaccine the plethora of these T-Cell responses are absent. Researchers are already aware that the T-Cell response plays a cooperative role in either the development of, or absence of, the ADE response.
Based on these differences and the skewed immunological response which is inherent with vaccines, I believe that the risk of ADE is an order of magnitude greater in a vaccine-primed immune system rather than a virus-primed immune system. This will certainly become more apparent as COVID-19 progresses over the years, but the burden of proof rests on the shoulders of the vaccine industry to demonstrate that ADE will not rear its ugly head in the near term or the far term. Once a vaccine is administered and people develop antibodies to some misrepresentation of the virus, it cannot be reversed. Again, this is a problem that could manifest itself at a later date.
Although this article focused on the problem of ADE, it is not the only pathway or mechanism that could present a problem for people being infected after vaccination. Another pathway is governed by Th2 immunopathology, in which a defective T-cell response initiates an allergic inflammation reaction. A second pathway is based on the development of faulty antibodies that form immune complexes, which then activate the complement system a consequently damage the airways. These pathways are also potential risks for SARS-CoV-2.
Right now, the fatality rate of the virus is estimated to be approximately 0.26%, and this number seems to be dropping as the virus is naturally attenuating itself through the population. It would be a great shame to vaccinate the entire population against a virus with this low of a fatality rate, especially considering the considerable risk presented by ADE. I believe this risk of developing ADE in a vaccinated individual will be much greater than 0.26%, and, therefore, the vaccine stands to make the problem worse, not better. It would be the biggest blunder of the century to see the fatality rate of this virus increase in the years to come because of our sloppy, haphazard, rushed efforts to develop a vaccine with such a low threshold of safety testing and the prospect of ADE lurking in the shadows. I would hope (and this is a big hope), that this vaccine WILL NOT BE MANDATORY.
Hopefully, you now know a little more about the topic of Antibody Dependent Enhancement, and the real, unpredictable dangers of a coronavirus vaccine. In the end, your health should be your decision, not some bureaucrat’s that doesn’t know the first thing about molecular biology.




